What You Will Learn
After reading this note, you should be able to...
- This content is not available yet.
Note Summary
This content is not available yet.
closeClick here to read a summary
Definition of Terms
- SEX: Refers to the physical state of being either male or female, determined by the sex organs.
- GENDER: Refers to the socially constructed roles, behaviors, expressions, and identities of males and females.
- Nonbinary: A term for gender identities that are not exclusively masculine or feminine
- Cisgender: A term for people whose gender identity matches the sex that they were assigned at birth
- Genderfluid: A person who does not identify themselves as having a fixed gender
- Male and Female: Traditional categories of 'man' and 'woman'
- Transgender: A term for people whose gender identity differs from the sex that they were assigned at birth
- Gender Neutral: Not identifying with any gender
- Agender: Without a gender (often used as a synonym for genders like neutrois or null gender)
- Pangender: A non-binary gender defined as being more than one gender
- SEXUALITY: Defined as one's sexual feelings, thoughts, attractions, and behaviors towards other people.
Examples of Gender Identities
It’s important to note that this is not an exhaustive list, and there are many more gender identities and terms that people identify with.
Described by Masters and Johnson in 1966.
- Desire
- Excitement Phase (Arousal Phase)
- Plateau Phase
- Orgasmic Phase
- Resolution Phase
There are attendant physiologic changes in the male and female bodies through all these stages.
ICD-11
- Sexual Dysfunctions
- Sexual Pain Disorders
- Gender Incongruence
- Specifiers: Lifelong, Acquired, Generalised, Situational, Unspecified
Sexual Dysfunction - ICD-11
- Hypoactive Sexual Desire Dysfunction
- Sexual Arousal Dysfunction
- Male Erectile Dysfunction
- Orgasmic Dysfunctions
- Ejaculatory Dysfunctions - Early, Delayed
- Other Specified Sexual Dysfunctions
- Sexual Dysfunctions, Unspecified
Sexual Pain Disorders - ICD-11
- Sexual Pain-Penetration Disorder
- Other Specified Sexual Pain Disorders
- Sexual Pain Disorders, Unspecified
- Aetiological Considerations in Sexual Dysfunctions and Sexual Pain Disorders
Gender Incongruence - ICD-11
- Gender Incongruence of Adolescence or Adulthood
- Gender Incongruence of Childhood
- Gender Incongruence, Unspecified
Other Specified Conditions Related to Sexual Health
- Conditions Related to Sexual Health, Unspecified
Sexual Dysfunction
Is persistent impairments of normal patterns of sexual interest or response that usually manifest as lack or loss of interest/enjoyment of sexual activities, the inability to experience or control orgasm, or a physiological barrier to successful sexual intercourse.
Individuals may avoid sexual opportunities, feel inadequate, or find it difficult to talk about it.
Criteria for a Diagnosis of Sexual Dysfunction Include:
- Inability to participate in a preferred sexual relationship.
- Presence of the sexual dysfunction on (almost) all occasions.
- Duration of at least 6 months.
- Significant stress or interpersonal difficulties.
- Not accounted for by a physical disorder, drug treatment (or use), or other mental or behavioral disorder.
Types of Sexual Dysfunctions
Sexual Desire Disorders
-
Hypoactive Sexual Desire Disorder
- Most commonly diagnosed sexual dysfunction
- More common in women than men
- Little or no sexual interest or desire
- Cause unclear
- Not secondary to other sexual problems (e.g., dyspareunia or erectile failure)
-
Sexual Aversion Disorder
- Strong negative feelings, fear, or anxiety due to the prospect of sexual interaction;
- Of sufficient intensity to lead to active avoidance of sexual activity
-
Lack of Sexual Enjoyment
- Lack of appropriate pleasure, despite normal sexual responses and achievement of orgasm
-
Excessive Sexual Desire
- Presenting as a problem for individuals, partners, or carers (when sexual disinhibition occurs)
- Referred to as nymphomania (women) or satyriasis (men)
- Could be secondary to a mood disorder (e.g., mania), early stages of dementia, associated with learning disability, secondary to brain injury, or as a side-effect of some drugs
Sexual Arousal Disorders
Male Erectile Disorder or Erectile Dysfunction
- Persistent difficulty achieving or maintaining an erection sufficient to complete sexual activity
- May occur due to performance anxiety
- May have an organic cause
Female Sexual Arousal Disorder
- Persistent difficulties becoming sufficiently lubricated in response to sexual stimulation
- May have organic causes
- Usually has psychological causes, such as anger, resentment, or trauma
Orgasmic Disorders
Female Orgasmic Disorder
Could be anorgasmic or others.
Male Orgasmic Disorder
Includes:
- Delayed Ejaculation
- Retarded Ejaculation
- Ejaculatory Incompetence
- Premature Ejaculation
Sexual Pain Disorders
Dyspareunia
Occurs in both males and females.
Vaginismus
Causes
Psychological
- Relationship problems
- Life stressors
- Anxiety/depression
- Low self-esteem
- Sexual performance anxiety
- Excessive self-monitoring of arousal
- Feelings of guilt about sex
- Fear of pregnancy or sexually transmitted diseases (STDs)
- Lack of knowledge about sexuality/'normal' sexual response
- Previous significant negative sexual experience (especially rape or childhood sexual abuse issues)
Environmental
- Fear of interruptions (e.g., from children, parents)
- Physical discomfort
Physical
- Testosterone deficiency
- Use of drugs or alcohol
- Pain or discomfort due to illness
- Fatigue
- Recent childbirth
- Medical conditions like heart disease, diabetes, spinal cord injuries, hormonal problems
- Surgical complications
- HIV medications
- Antihypertensives
- SSRI (Selective Serotonin Reuptake Inhibitors)
Factors Related to the Partner
- Sexual attractiveness
- Evidence of disinterest
- Constant criticism
- Inconsideration
- Inability to cope with difficulties (especially sexual)
- Sexual inexperience/poor technique
- Preference for sexual activities that are unappealing to the partner
Treatment
Psychotherapy - Sex Therapy Approaches
Common Goals of Sex Therapy
- Change self-defeating beliefs and attitudes
- Teach sexual skills
- Enhance sexual knowledge
- Improve sexual communication
- Reduce performance anxiety
Sensate Focus Exercises - Masters and Johnson Approach
A series of specific exercises for couples, essentially a form of in vivo 'desensitization' to reduce sexual anxiety. Partners are encouraged to take turns paying increased attention to their own senses.
The Helen Singer Kaplan Approach
Combines behavioral and psychoanalytic methods.
Sexual Desire Disorders Treatment
Self-Stimulation Exercises combined with Erotic Fantasies
Techniques aimed at addressing sexual desire issues.
Enhancing Communication
Improving communication between partners.
Expanding Repertoire of Couple’s Sexual Skills
Introducing new sexual techniques to enhance intimacy.
Couples Therapy Sensate Focus Exercises
Utilizing sensate focus exercises within couples therapy to address sexual concerns.
Medications
- Testosterone Replacement Therapy
- Use of Anti-anxiety Medications
Sexual Arousal Disorders Treatment
Erectile Disorder
Sensate focus exercises are used to reduce performance anxiety.
Biological approaches to the treatment of erectile disorder include:
- Surgery (i.e., vascular surgery or penile implants)
- Medication (e.g., Viagra)
- Vacuum pumps
Female Sexual Arousal Disorder Treatment
- Sex Education
- Working on Problems in the Relationship
- Artificial Lubricants for Lack of Sufficient Lubrication
Biological treatments include:
- A vacuum pump used on the clitoris
- Medications (currently under investigation)
Orgasmic Disorders Treatment
- Sensate Focus Exercises to Reduce Performance Anxiety
- Use of the Female-Superior Position
Individual therapy, typically for women, involves directed masturbation programs which include:
- Education
- Self-Exploration and Self-Massage
- Giving Oneself Permission
- Use of Fantasy
- Use of a Vibrator
- Involvement of the Partner
Premature Ejaculation Treatment
- Partner Uses the Squeeze Technique
- Stop-Start Method
Biological approaches to the treatment of premature ejaculation include the use of psychiatric medications.
Sexual Pain Disorders Treatment
Dyspareunia
Treat causes such as infections.
Vaginismus
- Insertion of Vaginal Dilators of Increasing Size to Help Relax the Vaginal Musculature
- Woman Controls the Pace and Depth of Penetration
Psychological therapy may also be needed.
Disorders of Sexual Preference (ICD-10)
Paraphilias (DSM-IV)
Are disorders in which an individual is sexually aroused by inappropriate stimuli.
- Homosexuality was previously included, but this is no longer the case.
- High comorbidity with anxiety, mood, and substance abuse disorders.
DSM-IV Criteria:
- At least 6 months of recurrent, intense sexually arousing fantasies, sexual urges, or behaviors involving a particular inappropriate act or object.
- These fantasies, urges, or behaviors must cause clinically significant distress or impairment in social functioning.
ICD-10 Criteria:
Has less strict and less detailed criteria, referring to the particular object or act as being the most important source of sexual arousal or essential for satisfactory sexual response.
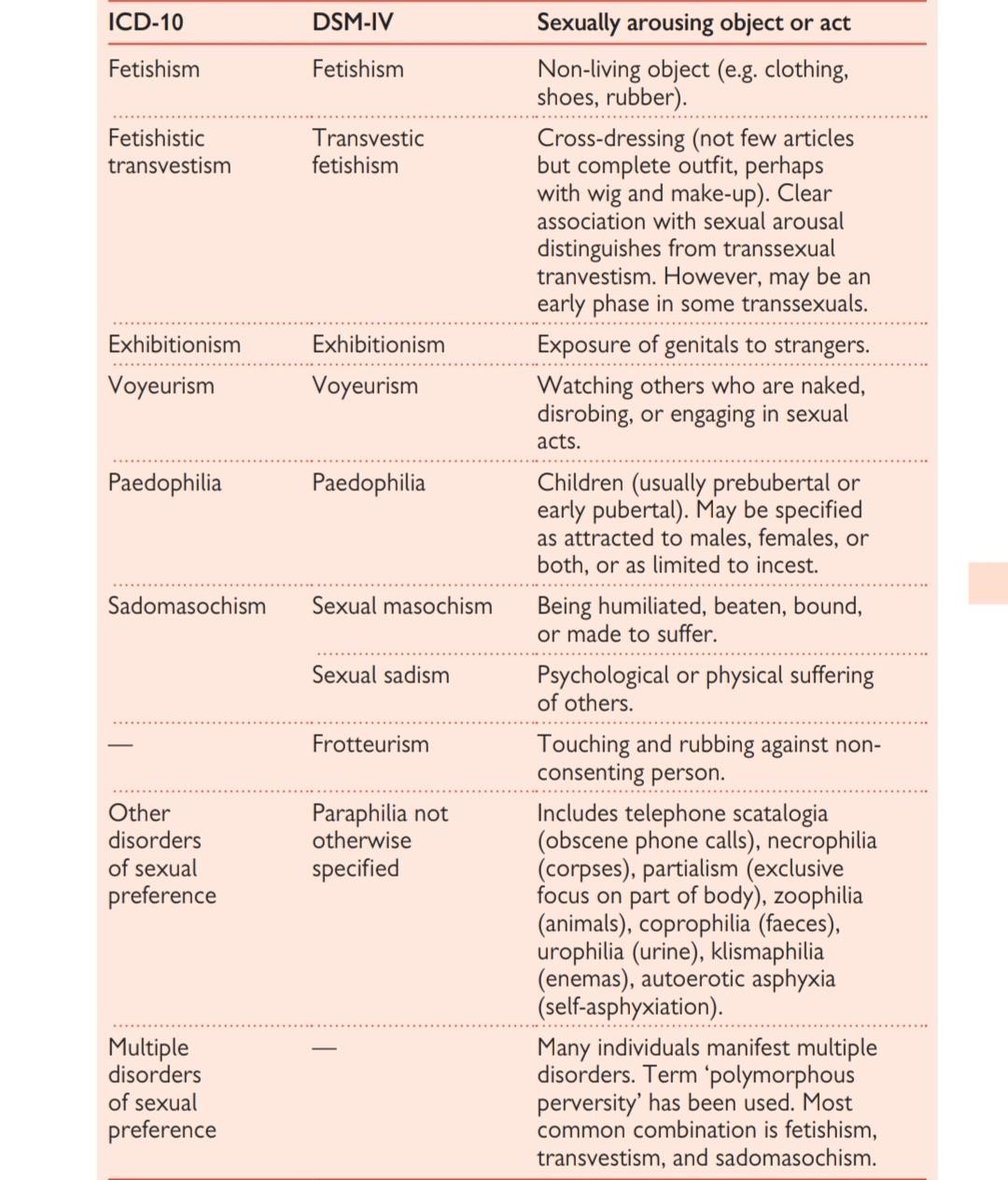
Classification of Disorders of Sexual Preference - ICD 10
- Fetishism
- Fetishistic Transvestism
- Exhibitionism
- Voyeurism
- Paedophilia
- Sadomasochism
- Other Disorders of Sexual Preference
- Multiple Disorders of Sexual Preference
Voyeurism
- Risk associated with "peeping" is necessary for sexual arousal
Exhibitionism
- Element of thrill and risk is necessary for sexual arousal
Relation Between Sadism and Rape
- Some rapists are sadists, but most do not show paraphilic patterns of arousal
- Rapists show sexual arousal to violent sexual and non-sexual material
Pedophilia
- Pedophiles: Individuals with a sexual attraction to young children
- Incest: Sexual attraction to one's own children
- Both may involve male and/or female children or very young adolescents
- Pedophilia is rare in females
- Incestuous males may be aroused to adult women; not true for pedophiles
- Most rationalize the behavior and engage in other moral compensatory behavior
Causes of Pedophilia
- Sexual and social problems and deficits
- Patterns of inappropriate arousal and fantasy may be learned early in life
- The role of high sex drive, coupled with suppression of urges
Psychophysiological Assessment of Pedophilia
- Assess extent of deviant patterns of sexual arousal
- Assess extent of desired sexual arousal to adult content
- Assess social skills and the ability to form relationships
TREATMENT
Psychosocial Interventions
- Most are behavioral and target deviant and inappropriate sexual associations
- Covert Sensitization – Imaginal procedure involving aversive consequences
- Orgasmic Reconditioning – Associate masturbation with appropriate stimuli
- Family/Marital Therapy – Address interpersonal problems
- Coping and Relapse Prevention – Teaches self-control and coping with risk
Medications: The Equivalent of Chemical Castration
- Often used for dangerous sexual offenders
Types of Available Medications
- Cyproterone acetate – Anti-androgen, reduces testosterone, sexual urges, and fantasy
- Medroxyprogesterone acetate – Depo-Provera, also reduces testosterone
- Triptorelin – A newer and more effective drug that inhibits gonadotropin secretion
Efficacy of Medication Treatments
- Drugs work to greatly reduce sexual desire, fantasy, arousal
- Relapse rates are high with medication discontinuation
Prognosis
- About 70% to 100% of cases show improvement
- Poorest outcomes are for rapists and persons with multiple paraphilias
- Most pedophilias run a chronic course and relapse rates are high
Gender Identity Disorder
- Transexualism
- Characterized by the desire to live and be accepted as a member of the opposite sex, usually accompanied by a sense of discomfort with one’s anatomical sex.
- Gender identity develops between 18 months and 3 years of age.
- Feels trapped in the body of the wrong sex. Most report that their gender dysphoria was present from early childhood. Karyotype and phenotypic development are normal.
- Transsexual identity should have been present for at least 2 years and must not be a symptom of another mental disorder, such as schizophrenia, or associated with any intersex, genetic, or chromosomal abnormality.
- TF to FTM ratio is 3–4:1
Differential Diagnosis
- Transvestism
- Fetishistic Transvestism
- Dual Role Transvestism
- Dysmorphobia
- Intersexed Condition
- Third Sex
- Schizophrenia
Treatment
- Psychological - Supervision of the transition, liaison with the primary care and surgical teams, and psychological support during the inevitable difficulties.
- Real-Life Test - At least 1 year before consideration of surgery
- Hormones
- Sex-Reassignment Surgery
- 75% report satisfaction with the new identity
- Female-to-male conversions adjust better than male-to-female
Practice Questions
Check how well you grasp the concepts by answering the following questions...
- This content is not available yet.
Contributors
Jane Smith
She is not a real contributor.
John Doe
He is not a real contributor.
Send your comments, corrections, explanations/clarifications and requests/suggestions